Those who develop digital offerings for health promotion or prevention often face the question: How can these be financed through health insurance companies?
Many software manufacturers are familiar with the reimbursement options available through DiGA. Much less well known is the monetization route via the Central Prevention Agency (ZPP). The Central Prevention Agency (ZPP) enables providers to have their digital courses (including those in the form of apps) certified so that they can be subsidized or reimbursed by health insurance companies. In this article, you will learn what requirements apply and what the path to successful ZPP certification looks like.
Even purely digital offerings, without personal course instruction, can be certified by the Central Prevention Agency (ZPP) under certain circumstances and subsidized by statutory health insurance companies.
Overview
- 1. Basis and background
- 2. What are digital prevention and health promotion services according to Chapter 7?
- 3. Formats of digital offerings
- 4. Distinction from DiGA (special chapter)
- 5. The four areas of action for prevention and health promotion
- 6. Criteria and guidelines for the certification of digital prevention and health promotion services by the ZPP
- 7. Benefits and cost-effectiveness of a digital prevention application
- 8. Further avenues for reimbursement by health insurance companies
- 9. Conclusion
1. Basis and background
The regulatory basis for the work of the Central Prevention Agency, which is jointly supported by all statutory health insurance funds, is the “Prevention Guidelines” of the GKV-Spitzenverband (National Association of Statutory Health Insurance Funds). The historical background to this was the realization that the healthcare system relies too heavily on purely curative measures, thereby neglecting (primary) prevention.
Section 20 of the German Social Code, Book V (SGB V) was created to specifically promote digital prevention services and thus contribute to promoting the health of insured persons and relieving the burden on the healthcare system. It obliges health insurance funds to support primary prevention and health promotion services and to promote corresponding offerings. On the basis of this paragraph, health insurance funds can cover all or part of the costs of certified prevention courses – provided that these comply with the GKV Prevention Guidelines and are recognized by the Central Prevention Agency (ZPP).
Originally, this path was probably designed more for courses offered by gyms and other course providers, for example. However, with growing awareness of the importance and opportunities of digitalization in healthcare, the need arose to create a framework for digital prevention services.
Digital formats were already eligible for reimbursement under Chapter 5, but only if they followed a traditional course structure with real-life course instructors, for example via video conferencing or online appointments. In 2020, one year after the introduction of DiGA, Chapter 7 was therefore added to the Prevention Guidelines. For the first time, this creates the basis for almost completely digital, self-directed prevention and health promotion services, i.e., programs that do not require direct course instruction and can be used independently by insured persons. However, instruction in the use of the app and personal support must still be provided by qualified persons.
2. What are digital prevention and health promotion services according to Chapter 7?
Digital prevention and health promotion services under Chapter 7 of the GKV Guidelines differ significantly in terms of content and form from traditional courses under Chapter 5. While Chapter 5 provides for a fixed course structure with modules that build on each other and a clearly defined sequence, Chapter 7 allows for flexible intervention design. Providers are free to design the content, sequence, and usage logic as long as the effectiveness and quality are proven.
There are also specific formal requirements. In addition to a coherent intervention and evaluation concept, evidence of data security, data protection, and quality assurance must be provided, for example through ISO certification. Chapter 7 thus creates the framework for modern, evidence-based, and technologically diverse prevention services that can be implemented independently in digital form.
However, while DiGA, for example, often manage entirely without human guidance, there must also be an option for personal support for otherwise digitally designed prevention services. The persons entrusted with providing support must be qualified for this task and are responsible for both introducing users to the service and answering individual questions.
3. Formats of digital offerings
The official guidelines basically distinguish between the following formats of digital prevention and health promotion services:
3.1 Internet interventions
Internet interventions, also known as online health training programs, are mostly behavior-oriented training programs that have been specially developed for use on the Internet. They are based on proven methods from traditional classroom training and have a clear structure. Participants are accompanied by a specialist who provides online feedback or answers questions. This support is referred to as “e-coaching” in the guide. Internet interventions typically consist of four to ten units, which are usually completed weekly via a web browser on a computer or tablet.
3.2 Mobile applications
Mobile applications, i.e., health apps, generally follow a training principle that focuses on the regular and usually daily performance of a specific health-related behavior. In contrast to internet interventions, which are completed after a set number of units, mobile applications are more aimed at permanently integrating healthy behavior into the everyday lives of users.
They often include functions for observing or measuring one’s own behavior and its effects, for example via digital diaries or sensors. The data collected can be used to define personal goals, provide motivational feedback, or reward progress.
Mobile applications are generally used on smartphones. There is usually no fixed structure in the form of completed training units, as they are used continuously and as part of everyday life.
3.3 Hybrid training concepts
Hybrid training concepts combine broader-based internet interventions with longer usage phases with mobile applications that are characterized by more frequent, shorter usage units. This allows structured learning units and everyday practice phases to be combined.
One example is digital stress management training, which consists of several interrelated learning and exercise units that are used on a weekly basis. This can be supplemented by a mobile app that allows users to do short relaxation exercises several times a day.
4. Distinction from DiGA (special chapter)
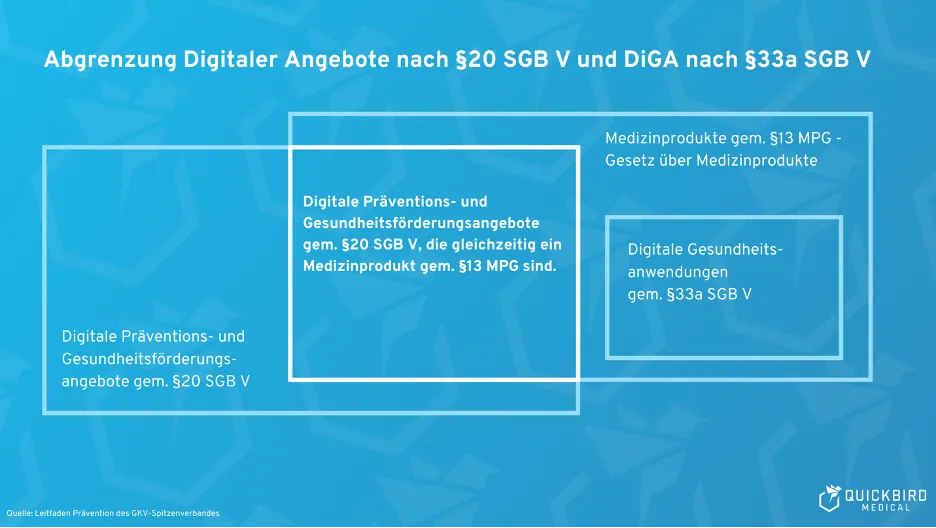
One of the distinguishing features of digital health applications (DiGA) is that they are not purely preventive measures. They are used to treat illnesses. Services certified by the ZPP, on the other hand, are intended to prevent illness.
In addition, DiGA are necessarily medical devices (risk class I, IIa, or IIb) according to MDR. Preventive services may also be approved as medical devices (see figure), but this is not a prerequisite for certification.
Find out more in our article on the topic of DiGA.
5. The four areas of action for prevention and health promotion
There are four areas of activity within which services are generally certifiable and reimbursable:
5.1 Movement habits
Exercise habits include, for example, measures that promote endurance, flexibility, and strength, reduce periods of inactivity (e.g., sitting), or increase the amount of time spent exercising. Fall prevention programs also fall into this category. In general, this refers to all programs that aim to increase physical and/or athletic activity.
5.2 Nutrition
Offers in this category aim to promote a varied and balanced—i.e., healthy—diet and encourage mindful eating. They also seek to promote the consumption of healthy foods and reduce the consumption of unhealthy ones.
5.3 Stress and resource management
Courses in this area aim to change the overall experience of stress and teach techniques for relaxation and coping with stress. This can be achieved, for example, through mindfulness exercises or by strengthening self-esteem and self-efficacy. Programs for improving sleep quality also fall into this category.
5.4 Addictive substance use
The field of action “Addictive substance consumption” deals with measures to reduce tobacco and alcohol consumption, for example. Here, for example, the frequency or quantity of consumption can be addressed.
6. Criteria and guidelines for the certification of digital prevention and health promotion services by the ZPP
Below, we explain the requirements you must meet and how the certification process works. You can find more detailed information on this in Chapter 7 of the Prevention Guide.
6.1 Health benefits
The health benefits are essentially what justify your product’s existence. They are derived from the field of activity in which your product is to be used.
Once your field of activity has been defined, you need to work out how your product can deliver added value in this area. You must then demonstrate this added value by means of a study (more on this below). You can find out which endpoints are permissible in the document Criteria for the certification of digital prevention and health promotion services.
Some examples of end points are:
- Increasing physical activity time (area of action: physical activity habits)
- Reduction in sugar consumption (field of action: nutrition)
- Strengthening self-esteem (field of action: stress and resource management)
- Reducing the weekly amount drunk (field of action: substance use)
6.2 Requirements for the study
The aim of the study is to demonstrate the effect of your offering over a specific period of time. One advantage is that comparison with a control group is not necessary (but of course not excluded); instead, an intra-individual comparison is sufficient. To this end, the defined endpoints are measured at specified times and compared with each other in order to evaluate the improvement achieved by your offering.
There is the possibility of provisional approval for an initial period of one year before full proof of health benefits is provided, provided that all other criteria are met.
If the study is successful, your application will then be approved by the Central Prevention Agency for three years.
6.3 Availability of individual support
Even if your offering is a web application or mobile app, personal support and availability are mandatory. This includes, in particular, user support for technical, content-related, and health-related issues. This can be provided by a single person (e.g., yourself) or a larger team. It is mandatory to ensure that the persons involved are qualified (e.g., by having the appropriate degree) and to provide documented training on the service.
6.4 Quality
Your offer must have a clearly defined target group and also point out possible contraindications. All statements regarding content, both in the application itself and in its marketing, must be substantiated by sources. For example:
- “Regular endurance training reduces your risk of a heart attack.”
- “Progressive muscle relaxation helps to reduce the experience of stress.”
- “Consuming social media before going to sleep reduces the quality of sleep.”
You are also responsible for ensuring that users understand how your service works. Please note that not only users of the service, but also any other persons involved (e.g., coaches) must be instructed accordingly.
6.5 User-friendliness and usability
The interface between humans and digital technology has long been a major topic. Entire fields of research deal with questions relating to the design of user interfaces. This also plays a central role in digital prevention services. The goals here are:
- High level of user engagement
- Positive user experience
This can be achieved, for example, through the use of gamification elements or through a wealth of interactive content.
An important source for implementing user-friendliness is, among other things, the ISO 9241 standard, which is explicitly referred to in the GKV guidelines.
6.6 Data protection & data security
In the area of data protection, it is important to implement the requirements of the GDPR as well as the requirements of German data protection laws such as the BDSG and SGB I. It is crucial to develop an understanding of what data your app processes and which other parties (processors) are involved.
Apart from data protection, data security (or information security) is also a key issue that should be given sufficient attention. The GKV-SV, for example, calls for the establishment of a certified information security management system (ISMS) in accordance with ISO 27001. In addition, you must comply with the BSI’s TR-03161 when developing the product. This is a “technical guideline” for the development of applications in the healthcare sector, which describes various aspects of data security.
6.7 Other legal requirements
Identifying and implementing additional legal requirements is fundamentally your responsibility as a provider. In addition to data protection regulations and the requirements of the Prevention Guidelines, this could include the Medical Device Regulation (MDR), for example. This is the case if your product is a medical device. Our blog article on this topic can help you determine whether your product is subject to the MDR.
6.8 Application and certification
Once development is complete, the certification process begins. This is handled via the online portal of the Central Prevention Agency (ZPP). Once you have created an account, enter your offer as a “course concept.” According to the ZPP, the review takes a maximum of 10 working days and is free of charge for you. Please note, however, that your offering and any persons involved (course instructors) will be reviewed separately. However, several review processes can be initiated at the same time.
The certification process can be restarted even after a rejection. The reasons for rejection should be communicated by the ZPP to enable you to make the necessary adjustments.
After successful certification, your course will be assigned a unique ID and added to the ZPP directory.
7. Further ways for reimbursement by health insurance companies
In addition to the Central Prevention Agency, there are several other ways in which software manufacturers can obtain reimbursement under the German healthcare system. These include, among others:
- Overview of all paths to reimbursement: Read our white paper
- Reimbursement for software in hospitals: Read our white paper
- Digital health applications – DiGA procedure: To our guide
- Selective contracts with health insurance companies: Our guide
- Reimbursement for software in the GKV medical aids directory (HMV): See our guide
- Digital care applications – DiPA procedure: To our guide
- NUB as cost reimbursement for software products in hospitals: See our guide
- Financing through the Innovation Fund: Our guide
- Public funding for digital health products: Our guide
8. Conclusion
With the framework for digital prevention and health promotion services, legislators have closed an important gap that left the concept of DiGA open as a purely curative application. The requirements for corresponding solutions have been appropriately relaxed compared to DiGA, but should not be underestimated.
Nevertheless, a digital course offering suitable for everyday use can be an interesting business model for course providers in addition to the health benefits for users.
QuickBird Medical offers a platform for digital health courses and develops customized prevention software solutions as needed. Please contact us if you are planning an app or web application in the field of prevention.