On December 19, 2019, the Digital Care Act (DVG) made it possible for doctors to prescribe digital health applications (DiGA) to patients in a standardized way for the first time.
With the Digital Care and Nursing Modernization Act (DVPMG), a counterpart to this was also created for nursing care in June 2021: digital nursing applications (DiPA).
DiPAs are designed to support the everyday lives of people in need of care and their environment through web and smartphone apps. For example, a digital care application could help to minimize the risk of falls for people in need of care or improve communication between relatives and carers.
The Regulation on the Assessment of the Reimbursability of Digital Care Applications (DiPAV) provides information on how the DiPA application process works and what requirements DiPA must meet in order to be included in the directory of digital care applications.
The Act on Expanding Authority and Reducing Bureaucracy in Long-Term Care (BEEP Act), which took effect on January 1, 2026, revised key provisions regarding DiPA. In particular, a one-year pilot period was introduced, the monthly reimbursement limit was raised, and the focus was expanded to include providing relief for caregivers.
In this article, we explain the difference between DiPA and DiGA, discuss the most important aspects of DiPAV, and ultimately provide a guide to the DiPA procedure. This guide outlines the process your application must go through in order to be included in the BfArM directory.
Table of Contents
- 1. Changes Introduced by the BEEP Act (in effect since January 1, 2026)
- 2. Distinction between DiPA and DiGA
- 3. Guidelines for DiPAV
- 4. Further ways to achieve reimbursement by health insurance companies
- 5. Conclusion
1. Changes Introduced by the BEEP Act (in effect since January 1, 2026)
The Act on Expanding Powers and Reducing Bureaucracy in Long-Term Care (BEEP Act) was passed by the Bundestag on November 6, 2025, subsequently referred by the Bundesrat to the Mediation Committee, and agreed upon in the mediation process on December 17, 2025. Following approval by the Bundestag and the Bundesrat (December 19, 2025), it entered into force on January 1, 2026. For DiPA, the Act contains the following significant changes, which have been in effect since then:
- A one-year trial period similar to the DiGA Fast Track has been introduced for DiPA. This requires a corresponding evaluation plan, as full evidence of benefit is not yet available. At the same time, the BfArM has eliminated the necessity assessment for supplementary support services.
- Reimbursement negotiations with the Federal Association of Long-Term Care Insurance Funds are taking place concurrently with the listing process. The right to care begins as soon as the reimbursement terms are agreed upon; if so agreed, it applies retroactively from the date of listing.
- The benefit entitlement for individuals in need of care is now up to 70 EUR per month (previously 50 EUR). Of this amount, up to 40 EUR is allocated to the DiPA itself and up to 30 EUR to supplementary support services. However, it should be noted that this monthly budget may already be exhausted after using a single DiPA. Since, in theory, multiple DiPA services can be used simultaneously, it may still happen under the new regulations that only the first use is reimbursed, and any additional DiPA services must be paid for out of pocket by the caregivers or the care recipients.
- The focus is on supporting caregivers: It is no longer mandatory for DiPA manufacturers to demonstrate a clinical benefit for the person in need of care. If the DiPA results in a reduction in the caregiver’s workload, it is assumed that this will have a positive effect on the person in need of care. To demonstrate this reduction in burden, an evaluation must be submitted. The law does not provide a definitive definition of what this evaluation should look like; further clarification is expected from the BfArM (likely in an updated version of the DiPA guidelines).
- DiPA are intended not only to provide relief, but also to help prevent the condition of people in need of care from deteriorating further — that is, to have a preventive effect and help maintain their existing level of independence.
- The use of DiPA remains limited to outpatient home care; its use in inpatient care is not planned.
Note: We will update this article on an ongoing basis as soon as the BfArM updates its DiPA guidelines to reflect the new legal situation or publishes further details (e.g., regarding evaluation concepts or negotiation frameworks).
2. Distinction between DiPA and DiGA
To better understand the digital care application, it helps to differentiate its use and content from the DiGA.
DiGA are apps that support sick people in the treatment, diagnosis, compensation or alleviation of illnesses, injuries and disabilities. Their use was recognized on December 19, 2019 with the DVG legally established. Since then, DiGA can be reimbursed by health insurance companies as part of medical and psychotherapeutic treatment. DiPA is a similar concept, but is primarily aimed at people in need of care. It was incorporated in mid-2021 through the Digital Care and Nursing Modernization Act (DVPMG) into the eleventh German Social Code (SGB).
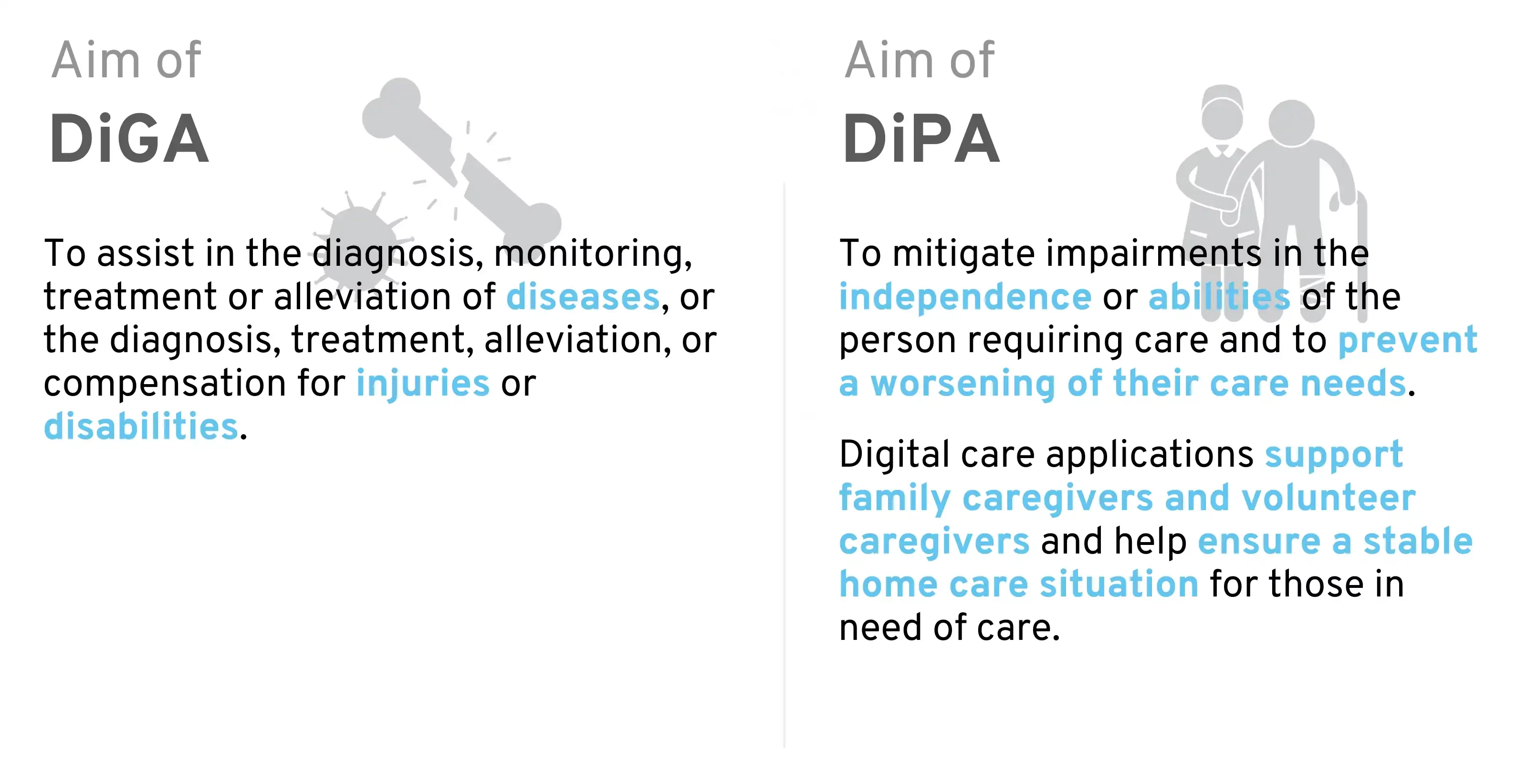
Distinction between DiGA and DiPA
As the distinction between DiGA and DiPA is not entirely obvious at first glance, we would like to highlight the most important differences in the following chapters.
2.1 Health insurance vs. social care insurance
The first major difference between DiGA and DiPA can be found in their place in the legal text. DiGA are defined in SGB V – Statutory Health Insurance, DiPA in SGB XI – Social Care Insurance. A DiGA is therefore reimbursed by the health insurance fund, whereas the costs of a DiPA are covered by the social care insurance fund.
A DiGA is prescribed by doctors and psychotherapists and is specifically designed to help people with certain medical conditions with pain relief, treatment, and diagnosis. To have a DiGA reimbursed by health insurance, a prescription from a doctor or psychotherapist is required, similar to the process for medications. Direct approval from the health insurance provider is also possible. A digital care application, on the other hand, can only be requested by those in need of care from their long-term care insurance provider.
The provision of a DiPA is approved by the long-term care insurance fund upon application by the person in need of care. The initial approval must be limited in time and may not exceed six months. Within this period, the long-term care insurance fund checks whether the digital care application has actually been used and whether the purpose of the DiPA is being achieved in the specific care situation.
If this review shows that both requirements are met, a permanent permit shall be issued. A new application is not required for this.
An indefinite authorization means that the long-term care insurance fund will provide a monthly reimbursement of up to 70 EUR (of which up to 40 EUR is for the DiPA and up to 30 EUR for supplementary support services; see Section 2.3) on a permanent basis, as long as the statutory eligibility requirements are met.
2.2 A DiPA does not have to be a medical device
§ 40a Digital care applications SGB XI:
“(1) People in need of care are entitled to care with applications that are essentially based on digital technologies”
§ 33a Digital health applications SGB V:
“(1) Insured persons are entitled to care with low-risk class medical devices whose main function is essentially based on digital technologies […].”
These are the introductory words of both paragraphs in the legal text, which immediately make it clear that there is a big difference in terms of the requirements for the digital care application.
While DiGA are explicitly defined as Class I, IIa, or IIb medical devices, DiPA are simply referred to as “applications.” A DiPA may be a medical device, but it is not required to be one. As a result, many of the regulatory requirements that DiGA manufacturers must navigate are (at first glance) not relevant to many DiPA.
However, the BfArM imposes similar requirements on DiPA that are not medical devices. For example, manufacturers must have a quality management system in place and meet requirements regarding the app’s safety and functionality. The BfArM’s current DiPA guidelines (Version 1.2, as of October 11, 2023; a version adapted to the BEEP legal framework is expected) therefore reference numerous ISO/IEC standards for medical devices and frequently cite the Medical Device Regulation (MDR). Thus, in most cases, the requirements for DiPA do not differ significantly, as they are based on the requirements for medical devices under the MDR.
If it is a medical device, it must belong to a low risk class (I or IIa). Unlike DiGA, DiPA is currently still not eligible for Class IIb.
If your application is to be certified as a medical device, you can find further information here.
2.3 Price cap
While the price cap for digital health applications (DiGA) is based on other applications in the same category, a fixed price cap is set for digital care applications. This stipulates that, since the BEEP Act took effect on January 1, 2026, up to 40 EUR per month can be reimbursed for the digital care application (DiPA), plus an additional 30 EUR per month for supplementary support services. In total, this amounts to up to 70 EUR per month (Section 40b of SGB XI in its current version; previously a uniform upper limit of 50 EUR). In principle, a DiPA may also be more expensive, but any additional costs must then be borne by the DiPA user.
Important from the manufacturer’s perspective: The new €40 limit under Section 40b(1)(1) of SGB XI is an exclusive cap on the DiPA itself. Up to €30 under No. 2 is earmarked for outpatient care facilities (Section 39a of SGB XI) and cannot be redirected to the manufacturer. Furthermore, these are reimbursement caps set by the long-term care insurance fund, not the provider’s price. The actual monthly reimbursement amount for your DiPA is negotiated individually with the Central Association of Long-Term Care Insurance Funds and may also be less than 40 EUR.
2.4 Can a DiPA also be a DiGA?
In principle, an application can be both a DiPA and a DiGA. The current status for manufacturers is that both applications can be submitted for one and the same app. However, deviations in the requirements must be noted. If a listing in both directories is achieved, the consumer’s service provider must check individually which health insurance fund will reimburse the application.
3. Guidelines for DiPAV
We have the contents of the DiPAV summarized in the form of a guideline, which clearly explains the application as well as the requirements and their proof. Particularly important is the Proof of the nursing benefits, which is also explained.
3.1 Requirements for DiPA
The requirements are listed in the legal text at an abstract level. Central assistance is provided by the Appendices 1 and 2 of the DiPAV, as well as Appendix 1 of the DiGAV, as these contain checklists that manufacturers can use to check the individual requirements for their product.
The following requirements apply to DiPA:
- Safety functionality (see DiPAV Annex 1): A distinction is made between medical devices and non-medical devices. Medical devices fulfill the requirements for safety and functionality through the CE conformity marking. Non-medical devices must fulfill the requirements according to Annex 1 of the DiPAV, which are very similar to the medical device requirements for risk class I, however. This requires, for example, the establishment of a quality management system for medical devices (e.g. in accordance with ISO 13485), as well as a risk management system.)
- Data protection and data security: In addition to the GDPR and the general state of the art in data security, the requirements specified by the BSI and the data protection test criteria defined by the BfArM for DiGA and DiPA must be fulfilled. In addition, all requirements from Annex 1 to the DiGAV must also be met for DiPA. However, as some of these points are not transferable 1:1, the BfArM’s DiPA guidelines provide further information on how to deal with these.
- Quality requirements: (see DiPAV Annex 2)
- Interoperability: Similar provisions apply here as for DiGA. Interoperable data export must be available in both machine-readable and human-readable/printable formats. The DiPA must also allow for the integration of medical devices used by users, provided that data from those devices is required.
- Robustness
- Consumer protection
- Age-appropriate usability, user-friendliness and accessibility
- Support for people in need of care and users
- Quality of care-related content
- Safety of those in need of care (patient safety)
- Clinical benefits or, alternatively, evidence of reduced caregiver burden
What is a nursing benefit?
A DiPA is considered to provide a care benefit if its use helps counteract a decline in the independence or abilities of the person in need of care. This also includes the progression of a person’s need for care. Furthermore, since January 1, 2026 (BEEP Act), a preventive effect — that is, the stabilization of existing independence before a deterioration occurs—has also been explicitly recognized as a nursing benefit.
In addition, there must be a nursing benefit in at least one of the following areas:
- Mobility
- cognitive and communicative skills
- Behavioral and psychological problems
- Self-catering
- Coping with and independently managing the demands and stresses associated with illness or treatment
- Organization of everyday life and social contacts
→ In addition to these areas, the care benefit can also be given in the area of household management.
It is important to note that DiPA users do not necessarily have to be the person in need of care themselves. Even if If caregivers are supported in providing assistance in one of the above-mentioned areas through the application, there is a nursing benefit.
Alternative since BEEP: Evidence of reduced burden on caregivers
Under the BEEP Act, it is no longer mandatory to demonstrate a benefit to the care recipient. Alternatively, a DiPA may be included in the directory if it results in a measurable reduction in the burden on caregivers—the legislature assumes that such a reduction indirectly has a positive effect on the care recipient. Manufacturers must submit an evaluation for this purpose; the methodological requirements are expected to be specified in an updated version of the BfArM DiPA guidelines.
Admissible studies to prove the nursing benefit
In order to demonstrate the nursing benefits, manufacturers must submit comparative studies. These may also be retrospective comparative studies, including retrospective studies with intra-individual comparisons.
Alternatively, prospective studies—and particularly randomized controlled trials—are recommended due to their high level of validity. The studies should be conducted in Germany. If this is not possible, their applicability to the German healthcare context must be demonstrated.
According to publicly available information, no DiPA had been permanently added to the registry by the time the BEEP Act took effect. Lindera’s widely discussed application in 2024 was rejected by the BfArM. According to Lindera’s press release, the BfArM criticized, among other things, that the submitted study could not demonstrate the app’s effects in isolation from existing care services. With the possibility of provisional inclusion as part of the trial year (see Section 3.2), the starting point for manufacturers could improve.
3.2 Application
Application procedure
The application for inclusion in the DiPA directory is submitted by the manufacturer to the Federal Institute for Drugs and Medical Devices (BfArM).
14 days after receipt of the complete application documents, the BfArM confirms receipt of the documents to the applicant or requests missing documents. The manufacturer has up to three months to complete missing documents. If no complete application documents have been submitted by the end of this period, the application will be rejected.
Once all documents are complete, the BfArM normally has 3 months to review the application and come to a decision regarding inclusion in the DiPA directory.
New as of January 1, 2026: Provisional admission during the trial year
Under the BEEP Act, manufacturers have access to a pilot testing procedure similar to that for DiGA: DiPA products may be provisionally included in the directory for up to one year if complete evidence of benefit is not yet available at the time of application. A prerequisite is a robust evaluation plan designed to demonstrate the nursing benefits or the reduction in the burden on caregivers during the pilot year. The BfArM’s assessment of the necessity of supplementary support services is no longer required. Reimbursement with the Federal Association of Long-Term Care Insurance Funds can be negotiated in parallel with the procedure and applies retroactively from the date of (even provisional) inclusion in the directory.
Content of the application
As of January 1, 2026, manufacturers may decide whether to apply for permanent inclusion or (if full proof of benefit is still pending) provisional inclusion as part of the pilot year. For permanent inclusion, all evidence (including evidence of care benefits or relief for caregivers) must be available at the time of application. For the trial year, an evaluation plan is sufficient. The application includes:
- Electronic application via the BfArM application portal
- Documents Demonstrating the Benefits of Care – for Applications for Temporary Admission – An Evaluation Plan
- Documents to prove compliance with all requirements
- Any additional documentation (e.g., instructions for use or, in the case of medical devices, conformity assessment according to MDR or MDD)
The manufacturer must also provide the following information in the application (according to §2 DiPAV):
- Manufacturer and identifying features of the DiPA
- The intended purpose
- Associated notified body (if applicable)
- Certificates issued by the notified body and the manufacturer’s declaration of conformity (if applicable)
- Instructions for use
- Purpose, mode of operation, content and use of the DiPA in a generally understandable form
- DiPA functions
- Institutions and organizations involved in the development of DiPA (if applicable)
- Sources for the nursing-related content and procedures implemented in the DiPA, in particular nursing-medical guidelines and expert standards, textbooks and studies
- Evidence of clinical benefit or relief for caregivers, including supplementary support services provided by third parties (as described in “Evidence of Clinical Benefit” and “Studies Demonstrating Clinical Benefit”), presented in a simple and easily understandable summary
- Group of people in need of care for whom a nursing benefit has been proven
- Care benefits that have been demonstrated for the specified group of care recipients and users
- Manufacturer-conducted study(ies) demonstrating the clinical benefits or the reduction in the burden on caregivers, including supplementary support services provided by third parties; if applying for provisional inclusion, the evaluation plan should be provided here
- Compliance with the requirements and guidelines for a DiPA, including the relevant questionnaires
- Intended user roles
- Quality-assured use of DiPA in the home environment, including exclusion criteria for use
- The type, content, scope and duration of the third-party support services required for the use of DiPA, if applicable
- Data processing locations
- Manufacturer’s compatibility commitments regarding supported platforms and devices as well as required accessories and other product components (if applicable)
- Standards and profiles used as well as human-readable export formats to create semantic, syntactic and technical interoperability
- Sum insured under the liability insurance taken out by the manufacturer for personal injury
3.3 Consultation from the BfArM
The BfArM advises manufacturers both before and after inclusion in the DiPA directory. The topics covered in the consultations are largely determined by you as the manufacturer. It is possible to clarify general questions of understanding regarding the DiPA requirements or to discuss product-specific documents.
For manufacturers whose DiPA is already listed, however, questions relating to the modification of the product can be dealt with.
The consulting fee ranges from €250 to €5,000 (admittedly a very wide range).
3.4 My DiPA is listed! What now?
Once the BfArM has issued a positive decision, your DiPA will be added to the registry. Congratulations—at this point, you’ve completed a major part of the work and can celebrate with your team. However, you’re not quite there yet: in addition to the listing, there are two more tasks to complete.
Negotiate remuneration with the National Association of Long-Term Care Insurance Funds
Within three months of listing, the reimbursement amount for your DiPA will be agreed upon with the Federal Association of Long-Term Care Insurance Funds. Since the BEEP Act took effect, you no longer have to wait until a positive decision is issued: reimbursement negotiations can begin even while the application process is still ongoing. If the two parties cannot reach an agreement, the arbitration tribunal will determine the price of the DiPA. Details regarding the arbitration process can be found in Section 8 (Paragraphs 30–32) of the DiPAV.
The right of persons in need of care to receive their DiPA benefits takes effect as of the date specified by the contracting parties in the reimbursement agreement (Section 40a(2), first sentence, of SGB XI); in practice, this is typically the date of inclusion in the directory, provided the parties so agree.
Clarify the technical and contractual framework
In addition, pursuant to Section 40a(4) of SGB XI, the technical and contractual terms for the provision of your DiPA must be established, including delivery methods, activation procedures, and cooperation with long-term care insurance funds.
3.5 Arbitration proceedings
The price for the DiPA is negotiated during the first three months negotiated between the manufacturer and the nursing care insurance fund after inclusion in the BfArM directory. If these two parties cannot reach an agreement, the arbitration tribunal determines the price of the DiPA. Details on the arbitration procedure can be found in section 8 (§ 30 – § 32) of the DiPAV.
4. Further ways to achieve reimbursement by health insurance companies
In addition to the DiPA procedure, there are also several other ways in which software manufacturers can obtain reimbursement under the German healthcare system. These include, among others:
-
- Overview of all paths to reimbursement: Read our white paper
- Reimbursement for software in hospitals: Read our white paper
- Digital health applications – DiGA procedure: To our guide
- Selective contracts with health insurance companies: Our guide
- Reimbursement for software in the GKV medical aids directory (HMV): See our guide
- Central Prevention Review Board (ZPP): About our guidelines
- NUB as cost reimbursement for software products in hospitals: See our guide
In addition to the aforementioned reimbursement options, it is also worth looking into public funding opportunities that can bridge the gap:
- The Innovation Fund: To the guide
- Many more subsidies for digital health products: To the guide
5. Conclusion
Meeting all the requirements for DiPA is no easy task. In particular, developing a robust evaluation concept — or, for permanent inclusion, providing proof of efficacy through a study — presents manufacturers with significant challenges. At least the long-awaited fast-track solution has become a reality with the BEEP Act as of January 1, 2026: DiPA can be provisionally included in the directory for up to one year, similar to the DiGA fast-track. Together with the recognition of caregiver relief as an equivalent means of proof and the increase in the monthly budget to up to 70 EUR, the framework conditions have thus been improved.
This guide is regularly revised to ensure that it is up to date.
QuickBird Medical develops DiGA, DiPA, and other regulated medical software for companies on a contract basis. If you are planning a product and need a partner for development and regulatory affairs, please feel free to contact us, and we will discuss your project with no obligation.